
A lot of what they tell us about viruses and vaccines is wrong. The rest is hidden (second part)

[ Here the transcript of the first part of the interview with Dr. Loretta Bolgan ]
We mentioned two of the three main immunopathological mechanisms: disease potentiation and cytokine storm. There is a third, the original unsanitary sin. Could you explain to us what it is and why it can be dangerous as an adverse effect of medium or long duration?
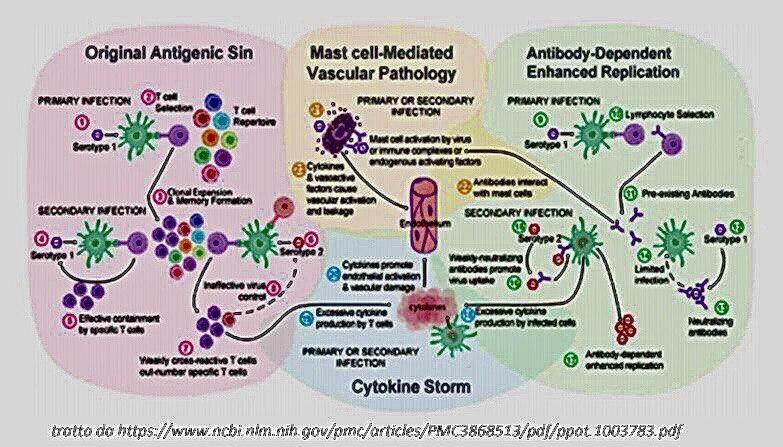
Yes, it always happens because weakly protective antibodies are formed. This has also been seen for diseases such as flu, measles, whooping cough and others. This is a rather well known and studied mechanism. It happens that following vaccination the immune system acquires a memory towards the vaccine antigen which directs the immune system in an unbalanced way towards the formation of antibodies. The immune system, in fact, usually activates completely when a virus arrives that causes damage : it activates the cytotoxic and antibody parts in order to eliminate or contain the virus and, finally, the damage repair phase. In the case of vaccines there is only the phase with the production of antibodies . The immune system, upon encountering the vaccine antigen, learns to respond by limiting itself to the production of antibodies. So what happens when the vaccinated person encounters the real virus, the one that produces the disease that can be serious and even fatal? Here, the circulating virus is recognized as if it were the vaccine antigen again and responds in the same way, i.e. by producing antibodies, but beware, the vaccine ones for which it has acquired memory due to the vaccine administered previously and therefore weak vaccine antibodies that do not they are able to block the mutated (circulating) virus . The virus then begins to replicate freely because it does not find resistance from the immune system, and the disease manifests itself in an atypical way with different symptoms than the reference disease, which can confuse doctors who do not understand that they are dealing with measles or a whooping cough because they start from the assumption that the person is vaccinated and therefore protected and does not have the typical symptoms of measles because for example it does not produce the typical red dots (rash) of measles and therefore we have an atypical form that can also prove resistant to treatments such as pertussis which becomes resistant to treatments and antibiotics . The disease tends to become chronic because the immune system is no longer able to completely eradicate it. If chronicity causes chronic inflammation, we understand what the risks are (the risk of autoimmunity). In other words, all these vaccination campaigns made to children, carried out with viruses that can cause an enhancement of the disease, lead to an exponential increase in autoimmune diseases in the adult population. With the Sars Cov-2 there are the conditions for the same dynamic to occur .
When in the near future adverse effects, even acute, should appear in the medium and long term, will it be easy to verify their etiology and attribute them to the mass vaccination campaign launched in this period? Will adequate epidemiological investigations be necessary, assuming that all the necessary data were available, to understand how things actually went?
Surely, if you do a post-hoc study to see if there has been an increase in the incidence of autoimmune diseases, before and after vaccination, we could have some indications. However, from experience I do not have great confidence in epidemiological studies because it is very easy to manipulate the data of the control group , in the sense that as a negative control group I have to have a large sample of a population that has never been vaccinated, healthy, and so far not has an epidemiological study of vaccines ever been done with a negative group of never vaccinated people . With pediatric vaccines, in fact, all epidemiological studies compare vaccinated populations with each other; even in the case in which it is a vaccinated population compared to another not vaccinated with the specific vaccine to be studied it is still a population vaccinated with all the other pediatric vaccines, so it is difficult, if not impossible, to understand which is the real one incidence of the disease . Even in the case of the COVID-19 vaccine, the same thing will happen. However, it is possible to investigate the type of autoimmune disease and the type of antibody that is causing it, provided they are antibody-mediated autoimmune diseases. That is, if we can find the autoantibodies that have been produced as a result of the infection, taking into account that our virus has very specific sequence homologies for certain human proteins, perhaps we can also make this connection. An explosion of autoimmune diseases is expected due to the molecular mimicry between SARS-CoV-2 and many human proteins, both of the central nervous system and of spermatogenesis . The phenomenon could explain the neurological problem that is already known, the brain fog or mental fog, suffered by those people who have been infected by the covid; the mediation of autoantibodies could also be at the origin of the onset of infertility problems linked to the infection. All these situations will be more evident when we go to vaccinate due to the mediation of vaccine antibodies . Another factor that must be taken into account is the massive production of bacterial toxins produced as a result of the intestinal microbiota infection , in this case long-term diseases could derive from a real chronic "poisoning" by toxins .
Missed pregnancies and neurodegenerative diseases affecting the central nervous system !?
Unfortunately, yes, there is already literature on a whole series of very serious central nervous system diseases, such as Guillain Barre, for example, Bell's palsy that we have seen among vaccine damage, multiple sclerosis, ALS , diseases also of the peripheral nervous system , all autoimmune diseases that could manifest themselves in the medium-long term after COVID and therefore it is very important to monitor those who have already developed the disease. The vaccine could aggravate or induce these diseases in susceptible individuals . As mentioned before, to know the true incidence of these diseases in the case of the vaccine, one must have an active long-term monitoring group of vaccinated healthy people, compared with an equally healthy group of unvaccinated and a negative group of never vaccinated. Surely this will not be done because they are already starting to vaccinate the unvaccinated control group . Therefore, the usual reactogenic adverse reactions to the vaccine will remain, i.e. acute reactions at the injection site and systemic reactions regarding fever and anaphylaxis, but longer-term ones will not be identified.
Recently an editorial by P. Doshi was published in the BMJ , who was finally able to examine the Pfizer-Biontech vaccination data and found that a large group of people, who after vaccination showed all the clinical symptoms of covid, did not it was counted simply because the swab on these people, despite the presence of symptoms, gave a negative result (false negatives). On the contrary, P. Doshi understanding these people and recounting the accounts found an efficacy of the vaccine between 19 and 29%, very far from the declared one (between 90 and 95%). He explains, therefore, that with these numbers the vaccine could not and should not be marketed resulting in the effective effectiveness below the minimum threshold of 50%. I ask for your comment and the difference between authorization and approval for a vaccine of this type.
It is evident that manipulation, especially in the control group, is very easy. And this is a problem that is found in all epidemiological clinical trials of vaccines. In order to verify it is necessary to go into the detail of the data that has been collected and it is not so simple because you have to ask for all the information that was used to make the assessments. What prof. Doshi is extremely serious because here we are talking about a manipulation of data , because the swab only gives a data relating to the presence of the virus but has no clinical diagnostic value and even if it was negative, they should have confirmed the covid 19 infection with the clinical diagnostics.
Could the serological test have been fine?
No, not even this is a valid test for the clinical diagnosis of COVID-19 disease, you should have done blood tests, lung CT, ect .; there are clinical analysis protocols that allow to confirm or deny the diagnosis regardless of the result of the molecular swab. In reality, serology does not give very reliable results even for laboratory diagnosis because it produces a significant rate of false positives. Therefore, the clinical diagnosis analyzes that must be done to frame the disease should be used. If they only selected patients on the basis of molecular testing, then they skewed all the results . Furthermore, having carried out the clinical study in the summer at a time when the epidemic was no longer there, it was not possible to do what is known as the “challenge test”, that is to verify how the vaccinated respond to the infection. It is obvious that they have not been able to tell if the vaccine worked or not, so that 95% is meaningless. The real meaning is that they don't know if it works or not. Not only that, but we do not know if at the time of the infection people will be protected or will enhance the disease .
With regard to authorization, we must take into account that the vaccine authorization procedures can be of three different types. That is, the ordinary marketing authorization, made following the normal registration process, therefore with the preclinical and clinical phase done consecutively. The EMA after the positive preclinical phase gives its approval for the trial to move to the first clinical phase on humans, from phase one to two, and two to three. Normally this process takes 10 years to reach the industrial scale production of the vaccine . In the case of the accelerated authorization with the Fast-Track, these phases are all done simultaneously so the clinical, preclinical and industrial production phases are compacted within a few months in order to be ready to then be able to produce the vaccine. Let's say that the industries have been extremely efficient on this, proving that they are actually able to market the product. This obviously comes at the expense of the vaccine's safety, quality and efficacy, but they felt that the urgency of having the vaccine was a priority . We now have conditionally authorized vaccines on the market. Conditional authorization means that the manufacturer has not yet finished the clinical studies and must continue to update the EMA on the results until the study ends . This is the meaning of conditional. When the conditional authorization period ends it will be marketed as a drug with a normal marketing authorization (MA). However, for the next five years the vaccine will remain experimental. There is another different procedure which is the emergency one that the FDA used to authorize the Moderna and Pfizer vaccines. To all intents and purposes this vaccine in America is experimental because they have not given any guarantees of efficacy or safety, while the EMA has stated that Pfizer has provided data that are sufficient to say that there is a positive benefit risk ratio. that is, the benefits would outweigh the risks. Unfortunately we cannot say that it is completely experimental based on the AIC that was given here in Europe, even if in fact it is … We know very well that the people who are getting vaccinated now are flocking to a clinical trial in progress …
Epigenetics is a relatively recent subject of study. Are there possible risks of altered gene expression among vaccinated people? Are there any risks of an epigenetic nature?
This is a risk that is generally run for all the vaccines we make, because we must bear in mind that it is either genetic material as in the case of attenuated viruses or proteins that are modified with formaldehyde, by binding with aluminum, or other . These vaccine antigens can lead to the production of peptides or viruses or part of viruses that can modify the epigenetic regulation of DNA, especially if the vaccine antigens are nucleic acids (DNA or RNA) . If you think of a vaccine like the adenovirus that goes beyond the nuclear membrane, enters the nucleus and localizes itself in an episomal position , that is, without integrating into the DNA, (at least not as a mechanism of action of the vaccine, but it could do so as an adverse reaction) it is inevitable that it interacts with DNA by silencing or activating certain genes, so the impact it may have on cell metabolism and DNA regulation is unfortunately unpredictable.
Is the vaccine that uses the adenovirus vector from Oxford-Astrazeneca?
Yes, as well as the Russian Sputnik5, and the Chinese Sinovac vaccine. These are particularly dangerous for various reasons. We take into account, in particular, that they have grown on immortalized fetal cell lines and therefore, unfortunately, there is a risk that we find these residues of transformed human genetic material and even cancer-causing viruses inside the vaccine .
Carcinogenic adventitious viruses among vaccine processing residues?
Yes, from cell lines. We consider that the purification of these vaccines is a very critical step and given the rapid lead times of large scale production it is easy to think that there will be quality problems. Unfortunately, there is no transparency for the part concerning quality due to the trade secret . A little more transparency can be found on clinical studies. If you make a request you can re-elaborate the data as did the prof. Doshi, but I have strong doubts about quality because I know that, at the time, companies had requested a facilitation for good manufacturing practices, that is, for the management of quality control of the production process. Facilitating actually means making fewer analyzes which could be detrimental to the quality of the finished product.
In the case of the Pfizer-Biontech vaccine it would seem that these criticalities cannot exist because they only use a fragment of the viral RNA, the one that codes for the spike protein. What are the most important critical issues in this case, starting with the oily PEG envelope?
The study on the toxicology of this vaccine I am doing now. I have studied it for now in a generic way so I reserve the right to answer after I have divulged the dedicated book (*). However, it must be said that the liposome that is used as a lipid carrier in nanoparticles already works as an adjuvant (substances that are added to vaccines to "enhance" the response of the immune system to the antigen) by stimulating the immune system in an inflammatory way . After entry into the cell and the release of the genetic material (the vaccine antigen) it should be understood how the latter is metabolized. It can be expected that the vector, being made up of lipid material, can stimulate certain distress signal receptors, mainly cytokines which are mediators of inflammation. The genetic material remains in the cytoplasm. It does not pass through the nuclear membrane and uses ribosomes there for the production of proteins. This is the theoretical and desired process, but the metabolism of the cells is not yet fully understood and specific studies have not been made that allow us to exclude the possibility that the antigen is transformed into other forms of genetic material . At the end of the vector there are modified, synthetic nucleotides. How the latter are metabolized we do not know. The other thing concerns the RNA fragment which is directly transformed into protein. It must also be said that when we go to inject this material, at the injection site there is an immediate activation of the danger signal because it is in any case foreign material, especially lipid, and nucleic acid that immediately activates a cytokine response. The cytokine storm is not really trivial because the most sensitive people could have very serious consequences in the face of an uncontrolled cytokine storm and we cannot even know what the longer-term consequences of the multi-organ damage to which they may be. they can meet . However, it has already been reported that this vaccine is very reactogenic. We also talk about anaphylaxis but it should be seen that they are not cytokine storms caused by the aforementioned mechanism.
I think this vaccine used by Pfizer is not suitable for large-scale use at all. It really has big management problems, the expiration time is too short, six months is not enough to administer such a vaccine in hundreds of millions of doses. To do it well it would take an extremely efficient structure that we do not have. The vaccine must be strictly stored at 80 ° C below zero to avoid degradation which would, on the one hand, reduce the amount of vaccine antigen, and therefore would compromise the theoretical efficacy of the vaccine, but on the other also lead to production of degraded lipid material and nucleic acid which works as a powerful adjuvant, but in the negative sense, because it can cause an excessive inflammatory effect, thus increasing the potential adverse reactions.
Is it important that the cold chain for this kind of vaccine is completely intact?
Absolutely yes, otherwise it degrades very quickly. Degradation significantly increases the incidence of adverse cytokine storm reactions.
Is it possible to interpret what happened in Norway, I am referring to the 23 deaths, then 29, following the vaccination of many elderly users of a nursing home that hosted them, in the light of what we are discussing, anaphylactic shock or other?
It could have been a potentiation of the fatal disease, or a systemic allergic reaction, i.e. anaphylaxis, as well as the consequence of an uncontrolled cytokine storm. A vaccine that already has these problems of its own, when administered to patients who have no ability to counteract the damage caused by the vaccine, can obviously result in a fatal complication. It is said that it is normal because they were elderly people with multiple pathologies, but the question to ask then is, if you knew from the beginning that they were fragile people and therefore at risk of fatal damage why did you vaccinate them? Vaccination is not euthanasia… Following their logic according to which vaccine deaths are not worrying and negligible, then covid deaths should also be considered not worrying and negligible. So let's put the concern reserved for deaths on the same level, because if you die from vaccine damage the event should not be considered worrying, vice versa it is unacceptable if you die from covid . This usually happens in the case of children who develop vaccine complications due to previous diseases or genetic predispositions. When a child with health problems, even potential ones (the famous genetic mutation not yet discovered …) is vaccinated and the complication intervenes, this is automatically charged to the current or presumed disease and not to the vaccine. A child, with other medical conditions underway, who makes measles dies of measles. Another with the same pathology, if he gets the vaccine and dies from the vaccine it is said that it was not the vaccine that killed him but the pathology. This kind of tricks are used all the time.
One last question (then when will complete the study that announced us about mRNA vaccines, if you can, I would be happy to be able to find ourselves talking about it). The vaccination campaign has started in the UK and data are already available, around the incidence, of 2.79% of short-term adverse effects among vaccinated people who according to the CDC report needed hospital treatment . A very high percentage that, in the unfortunate event, in which all Italians were vaccinated, would produce one million and six hundred thousand patients who would need hospital care immediately after the vaccine. What do we know, to date, about the short-term adverse effects of the vaccination campaign already started and where it is possible to monitor what is happening to the vaccinated population?
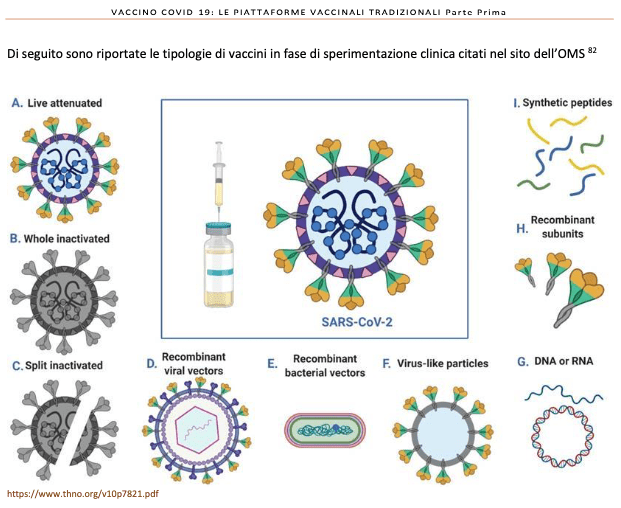
By law, the pharmaceutical industries and regulatory agencies should collect the data from the reports through the pharmacovigilance system. However, adverse reactions are currently collected through passive reporting from the vaccinated population (VAERS in the USA), because active pharmacovigilance, which includes medical examinations and any analyzes on the person to investigate any adverse reactions, usually does not go beyond a week because only the reactogenic reactions to the vaccine are collected, not the medium and long term ones . The serious reactions that could develop in the medium and long term could also risk losing them as information or being underestimated by up to 90% as happens for other vaccines. Acute adverse reactions that occur early, yes, should definitely be recorded. Once the damage has been ascertained, the motivation should be studied, what caused it, because it is essential to be able to intervene. An anaphylaxis is different from a cytokine storm and needs to be treated differently, so potentiation of the disease is an additional mechanism. It is therefore a question of developing the right therapeutic strategies that will be fundamental to save the life of the people who may be victims. If they do not study this kind of reactions and the related data are collected passively without going to verify the causes and mechanisms by which they occur, there is a risk that people will die without being able to know the reason for the deaths . Maybe the autopsies and other investigations are not carried out that would allow us to understand if the cause of death can be attributed to the vaccine or not, and what we have not been able to know we say remains hidden, it simply does not exist: the damage is denied because the data is missing . This is another very serious thing that is a constant of vaccinations. In the book that I hope will be released in a few days (*) I have explored all the traditional vaccination platforms because the innovative platforms with nucleic acids and therefore that of GMO vaccines are a small part of the vaccines that will be put on the market. We take into account that at the end of December we had 289 different vaccines undergoing preclinical and clinical studies , of which 66 are being revised to obtain marketing authorization. Most of these are traditional vaccines. Only one with attenuated virus, in the form of nasal spray that they are testing in England, different viruses inactivated with classical adjuvants, those with protein subunits, those with viral-like particles, and then the large category of nanoparticle or nanovaccines, so these are the categories that we will have to face. The large part is to proteins not to nucleic acids. Here are all the problems related to the technology and the type of virus that is used because the big problem, in addition to the technology, are the particular characteristics of the Sars-Cov-2.
A note on the flu shot. We must think that the problem we are seeing for this vaccine, authorized with an accelerated procedure, is actually also valid for the flu vaccine, which is authorized in the same way every year and is a vaccine that is administered on a very large number of the population. worldwide. There are vaccines such as Vaxigrip, of which, since the 1980s, billions of doses have been administered with a one-week pharmacovigilance, performed annually on an average of 20 people and for which, in reality, reliable data on the incidence are still lacking. of long-term adverse reactions. Today we are all focused on the sars cov-2 vaccine because it is new, because it is GMO etc. but mandatory pediatric vaccines do not enjoy a better benefit / risk assessment; even less is the anti-flu one which entails the risk of the enhancement of the disease which is totally ignored. It is administered in particular to elderly people and therefore predisposed to harm and pharmacovigilance is not done as it should be done. In short, we are not discovering anything new …
I take this opportunity to ask you how often the emergency procedure called "fast-track" is applied? Is this sort of preferential lane also granted for the production of other drugs?
Yes, I have seen that fast track (FT) was initially introduced to produce vaccines and emergency drugs; for example the Ebola vaccine, certain HIV drugs or cancer drugs, all drugs that have a certain emergency because their demand from the population is very high. The FT relies heavily on demand from the people. They justify granting a facility to producers because people would ask for it. It is the social context that leads producers to apply for the concession of the FT abbreviated procedure. It has been used more and more frequently. If I remember correctly, the FDA's position to accelerate the authorization with this type of procedure is in 2018. We take into account that we have more than 600 experimental drugs for covid in FT . So not only the vaccine but also all the experimental drugs, which is why the WHO urged not to use hydroxychloroquine (used for other diseases), as well as to block the testing of off-label drugs (eg Adenosine and others ) because there are all the precision experimental drugs, that is, designed only for SARS-Cov-2, in the course of a clinical trial that will be progressively authorized with the FT .
So be careful because in addition to the vaccine we will have to deal with many experimental drugs, among all monoclonal antibodies which are the other large category of biological drugs with similar problems of quality, safety and efficacy of vaccines .
Warning
Anyone interested in the scientific literature on which Dr. Loretta Bolgan's arguments are based can find the relevant documentation on her website studiesalute.it/salute, in particular in the Covid-19 / vaccine section.
(*) The book, to which Dr. Bolgan refers, is also now available in the Covid-19 / vaccine section .
Here is the transcript of the first part of the interview with Dr. Loretta Bolgan
![]()
Thanks to our Telegram channel you can stay updated on the publication of new articles of Economic Scenarios.
The article A lot of what they tell us about viruses and vaccines is wrong. The rest is hidden (second part) comes from ScenariEconomici.it .
This is a machine translation of a post published on Scenari Economici at the URL https://scenarieconomici.it/moltissimo-di-cio-che-ci-dicono-su-virus-e-vaccini-e-sbagliato-il-resto-e-nascosto-seconda-parte/ on Thu, 04 Feb 2021 19:38:36 +0000.