
Sars-Cov-2, what will happen in the autumn-winter. Report Iss-Ministry of Health
The 7 unknowns and 4 scenarios of Sars-Cov-2 for autumn-winter in Italy according to the most updated report of the Ministry of Health in collaboration with ISS (Higher Institute of Health)
The scenarios in Italy for the autumn, in terms of impact on the health system, will depend a lot on some unknowns:
1) Transmission of SARS-CoV-2 in late summer. In fact, it is not yet clear whether the increase in transmissibility (Rt) observed starting from June in some Regions / PA will stabilize around the values observed during the month of September or will continue to increase over time. It is quite evident that the scenarios will change considerably depending on whether or not it is possible to keep Rt at values close to 1 in the autumn-winter season.
2) Transmissibility of SARS-CoV-2 in schools. The true transmissibility of SARS-CoV-2 in schools is not yet known, although outbreaks in school settings are beginning to be described in countries where schools have been reopened longer. Furthermore, the impact that the school reorganization measures adopted may have has not been quantified. More generally, it is not known how much children, mainly asymptomatic, transmit SARS-CoV-2 compared to adults, although there is evidence that the viral load of symptomatic and asymptomatic, and therefore the transmission potential, is not statistically different. All this makes the role of transmission in schools as of September on the overall epidemiology of SARS-CoV-2 in Italy very uncertain.
3) Transmissibility of SARS-CoV-2 in the workplace. Workplaces have proved to be an important reservoir of infections since the acute phase, not only in specific risk environments, such as healthcare, but also in contexts that, in Italy and beyond, have also been characterized by clusters of considerable size , for example in the agri-food sector (farms, meat processing, markets) and in that of courier shipments. Furthermore, the resumption of work activities in the presence, even if in varying percentages depending on the sector, could contribute to the activation of further epidemic outbreaks.
4) Impact of population mobility on SARS-CoV-2 transmission. The resumption of school and work activities in presence tends to make the public transport system in general and, in particular, the local one, fully operational, with an inevitable increase in the opportunities for exposure to the virus.
5) Contribution of the company prevention system in the workplace. The system created over time has already revealed itself, with greater value than ever, as a natural infrastructure capable of contributing to the mitigation of risk, in light of the integration of organizational measures of prevention and protection envisaged starting from the "Shared protocol for the regulation of measures to combat and contain the spread of the COVID-19 virus in the workplace "of March 14 and its integration on April 24 and in the sector protocols, favoring – also for the autumn-winter period – the protection of health and safety of the 23 million workers involved, with inevitable positive effects also on the community. Health surveillance continues to be of particular importance, also in relation to risk information activities as well as for the protection of so-called “fragile” workers.
6) Degree of acceptance of sanitation and behavioral measures for the prevention of transmission of SARS-CoV-2 by the general population. For example, there are possible exacerbations of critical issues already encountered at the present stage, such as the collaboration of positive subjects for the conduct of epidemiological investigation and contact tracing activities and compliance with / adherence to default measures both for confirmed cases and for close contacts.
7) Response capacity of prevention and control systems. There is evidence of the improved ability of prevention systems to rapidly identify outbreaks, isolate cases and apply quarantine measures to case contacts, which is a major contributor to keeping transmission under control. However, it is not known at the moment what level of transmission, for example in terms of the number of outbreaks, that prevention systems can effectively manage. Finally, it should be considered how the beginning of the flu season can make these activities more complex and demanding.
Another important aspect to consider, related more to the health system's stability than to the transmissibility of SARS-CoV-2, concerns the average age of cases. In the summer months, a significant decrease in the average age of cases was observed with relatively few new hospitalizations from COVID-19, however, this was then followed by a new increase in the median age in cases diagnosed between late August and late August. beginning of September. It is currently unclear whether this trend will persist over time and whether it will be possible to keep risk categories such as the elderly protected.
In light of these unknowns, the possible scenarios that lie ahead for the autumn in the various regions can be summarized as follows:
• SCENARIO 1
Situation of localized transmission (outbreaks) substantially unchanged compared to the period July-August 2020, with regional Rt above the threshold for limited periods (less than 1 month) and low incidence, in the event that transmissibility does not systematically increase in early autumn , schools have a modest impact on transmissibility and regional health systems are able to track and control new outbreaks, including school ones.
• SCENARIO 2
Situation of sustained and widespread transmissibility but manageable by the health system in the short-medium term, with regional Rt values systematically and significantly between Rt = 1 and Rt = 1.25 (i.e. with estimates of the 95% Confidence Interval – IC95 % – of Rt between 1 and 1.25), in the event that new outbreaks, including school ones, cannot be fully tracked, but still manage to greatly limit the transmission potential of SARS-CoV-2 with ordinary and extraordinary containment / mitigation measures. An epidemic with these characteristics of transmissibility could be characterized, in addition to the evident impossibility of containing all the outbreaks, by a constant increase in the incidence of cases (at least symptomatic ones; it is in fact possible that a reduction in the percentage of asymptomatic cases is observed identified with respect to the total given the impossibility of carrying out the epidemiological investigation for all new outbreaks) and corresponding increase in hospitalization rates and admissions to intensive care. However, the growth in the number of cases could be relatively slow, without leading to a significant overload of care services for at least 2-4 months.
• SCENARIO 3
Situation of sustained and widespread transmissibility with risks of maintaining the health system in the medium term, with regional Rt values systematically and significantly between Rt = 1.25 and Rt = 1.5 (i.e. with 95% CI estimates of Rt between 1, 25 and 1.5), and in which the transmission potential of SARS-CoV-2 can be limited only modestly with ordinary and extraordinary containment / mitigation measures. An epidemic with these transmissibility characteristics is expected to be characterized by a faster growth in the incidence of cases than in scenario 2), a failure to track chains of transmission, and initial signs of overload of care services following the increase in cases of high clinical severity (with an increase in the occupancy rates of hospital beds – critical and non-critical area) attributable to a high or very high risk level based on the weekly monitoring system. The growth in the number of cases could lead to an overload of care services within 2-3 months. However, it is important to note that if the epidemic were to spread mainly among the younger age groups, as observed in the period July-August 2020, and it was possible to protect the most fragile categories (e.g. the elderly), the time margin within which to intervene could be greater.
• SCENARIO 4
Situation of uncontrolled transmissibility with criticality in the stability of the health system in the short term, with regional Rt values systematically and significantly higher than 1.5 (ie with estimates CI95% of Rt greater than 1.5). Even if an epidemic with these characteristics would lead to more aggressive mitigation and containment measures in the affected territories, such a scenario could quickly lead to a high number of cases and clear signs of overload of welfare services, without the possibility of tracking the origin of new cases. The growth in the number of cases could lead to an overload of care services within 1-1.5 months, unless the epidemic spreads predominantly among the younger age groups, as observed in the period July-August 2020, and managed to protect the most fragile categories (eg the elderly). In this regard, it should be noted that it appears rather unlikely to be able to protect the most fragile categories in the presence of an epidemic characterized by these values of transmissibility.
++++
Approach to the re-modulation of containment / mitigation measures at regional / PA level in the context of hypothetical scenarios of transmission of the SARS-CoV-2 virus on the national territory in the autumn-winter period
Pursuant to Prime Ministerial Decree No. 126 of May 17, 2020, the Regions and Autonomous Provinces are granted the authority to define the methods and timing of the various activities restored during the post lockdown reopening:
"Provided that they have previously ascertained the compatibility of the performance of the aforementioned activities with the trend of the epidemiological situation in their territories and that they identify the applicable protocols or guidelines suitable for preventing or reducing the risk of contagion in compliance with the principles contained in the protocols or in national guidelines "(114).
To support the assessment of the regional epidemiological situation, the Ministry of Health in collaboration with ISS has set up a system for monitoring the risk and resilience of health services on a weekly basis which is shared with the Regions / PA and evaluated by a control room set up by experts from the Ministry of Health, the ISS and a representation of the Regions / PA (29).
This section proposes a common approach to the scalability of the measures on the basis of the transmission scenarios described in the document hypothesized at national level in the awareness that very different epidemiological conditions can occur in each Region / PA, such as to provide for specific and non-uniform control / mitigation measures. on the national territory.
The measures set out in the scenarios have the function of supporting and orienting the decision-making process of the individual Regions and Autonomous Provinces in relation to their epidemiological scenario and, precisely because of their orientation function, they are not to be considered binding.
For each national scenario, scalable measures are therefore assumed based on the likely level of risk that could be identified in the weekly classification provided to each Region / PA based on the monitoring defined pursuant to the Health Ministerial Decree of 30 April 2020 (29) (e.g. not very low risk levels are considered likely to be in critical transmission scenarios such as scenario 4).
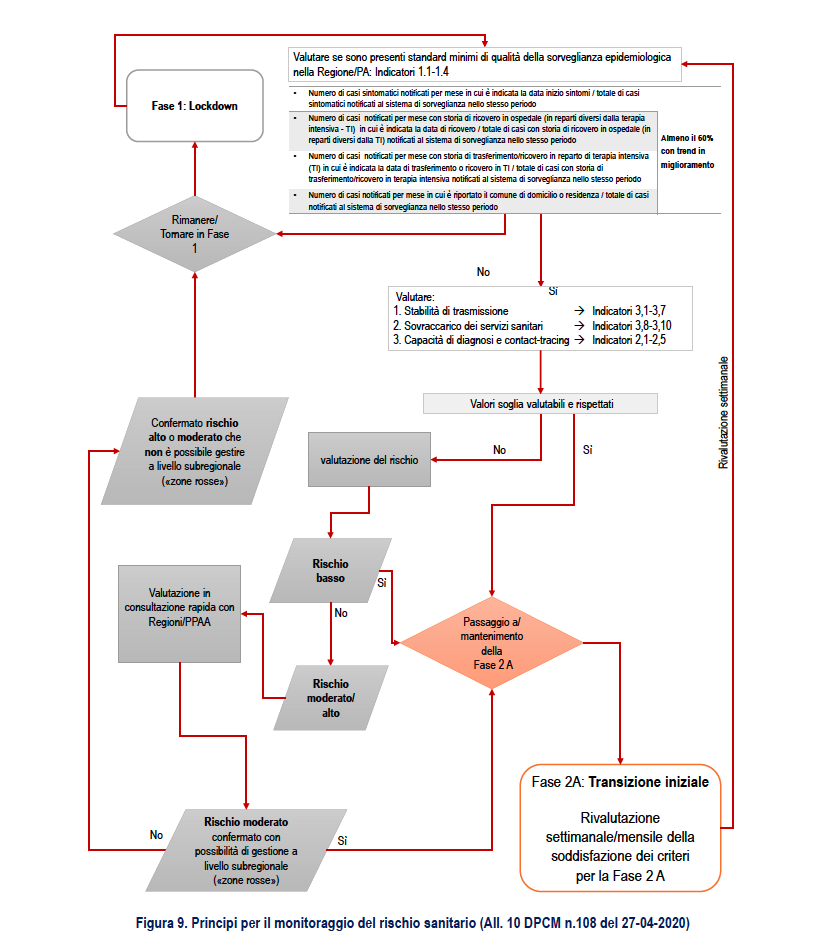
The proposed re-modulation both in a restrictive and in a permissive sense (escalation and de-escalation) is consistent with what is indicated in attachment 10 (28) "Principles for monitoring health risk" to the Prime Ministerial Decree of 26 April 2020 "Further implementing provisions of the decree-law 23 February 2020, n. 6, containing urgent measures regarding the containment and management of the epidemiological emergency from COVID-19 ", applicable throughout the national territory (Figure 9) which is described in more detail based on the transmission scenarios described in this document.
For the modulation in escalation and de-escalation of the measures, temporal criteria are set that take into account both the physiological delay of at least 3 weeks in the observation of epidemiological changes from the surveillance data and related to the incubation of the disease and the timing of notification / data transmission, and possible further delays in scenarios with higher transmission due to a significant increase in the number of cases to be reported such as to overwhelm the ability to maintain adequate levels of timeliness and completeness.
SCENARIO 1. Situation of localized transmission (outbreaks) substantially unchanged compared to the period July-August 2020
Scenario description 1
Regional RTs above threshold for limited periods (less than 1 month) and low incidence, with transmission mainly associated with identified outbreaks, in the event that schools have a modest impact on transmissibility and regional health systems are able to track and control the new outbreaks, including school outbreaks.
In a national scenario of this type, it is presumable that many Regions / PAs are classified as low or moderate risk, even if high risk situations are possible, perhaps at a sub-regional level.
1. Weekly Risk Rating: VERY LOW / LOW
Action: re-modulation of activities with less stringent measures (de-escalation) or maintenance
Interventions: ordinary, including:
• Case isolation
• Contact quarantine
• Standard precautions (PPE, physical distancing, individual / environmental hygiene) defined by the competent institutions (CTS, Ministries, ISS, INAIL etc.).
2. Weekly risk classification: MODERATE
Action: evaluate the re-modulation of activities with more stringent measures (escalation) or maintenance
Risk assessment in the Region / PA to define sub-regional situations of higher risk (circulation in the provinces / municipalities; school outbreaks)
Interventions: ordinary + extraordinary in single institutions (eg schools) or limited geographical areas
• Greater control of the actual implementation of the measures already adopted on the territory (see minimum criteria)
• Scaled precautions where indicated in the documents produced for specific areas and contexts (eg schools) only in areas with greater risk of exposure
• Possibility of closure of activities, suspension of events and limitation of population mobility in sub-regional geographical areas (municipalities / provinces)
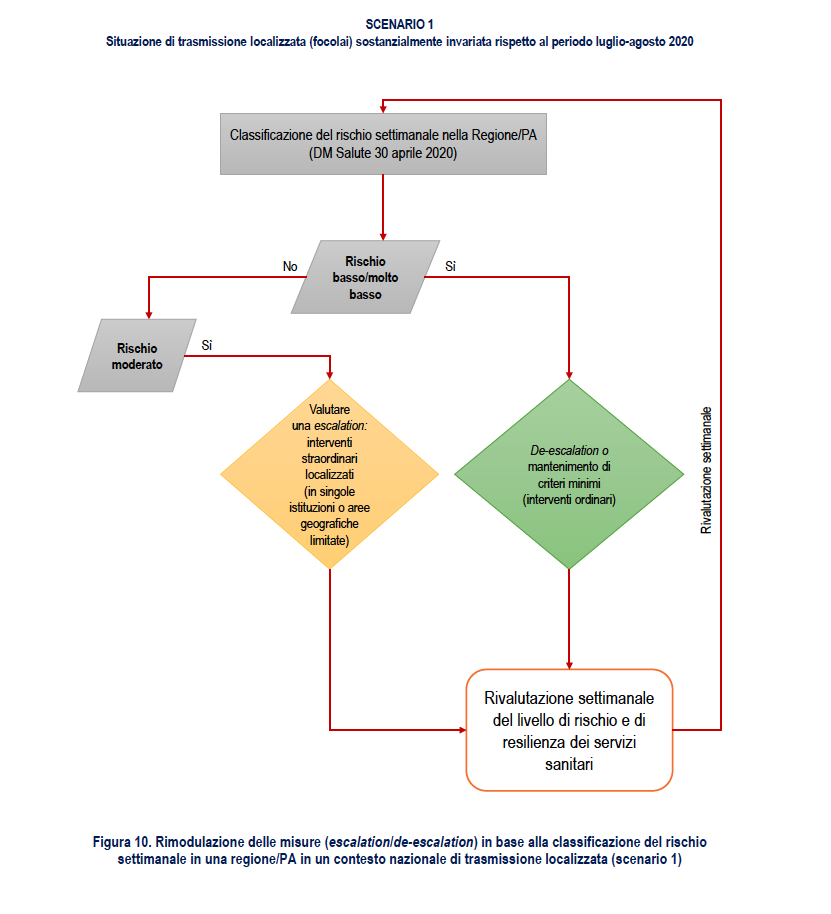
Figure 10 proposes a flowchart related to the re-modulation of measures based on the weekly classification of the risk in a Region / PA.
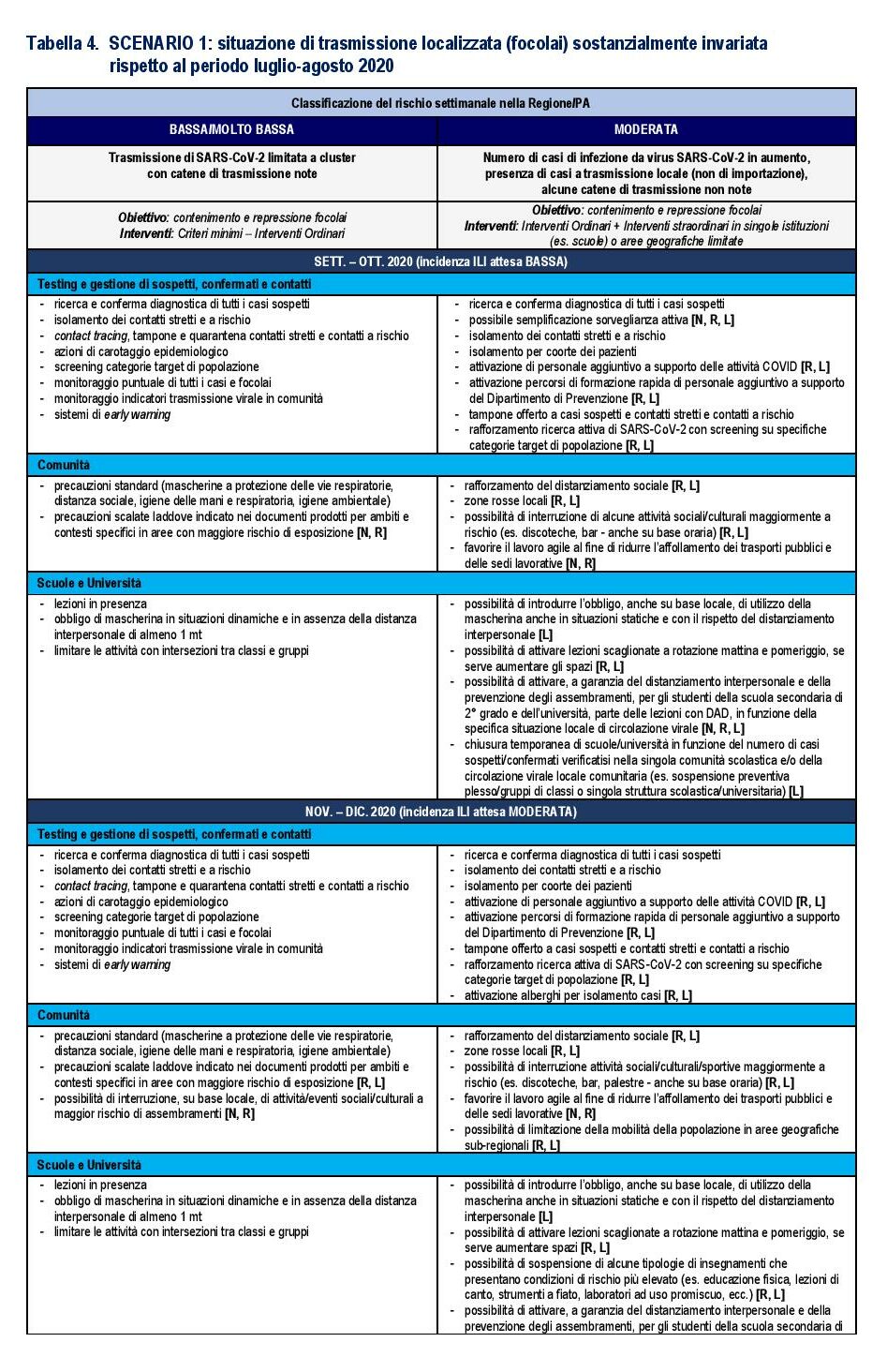
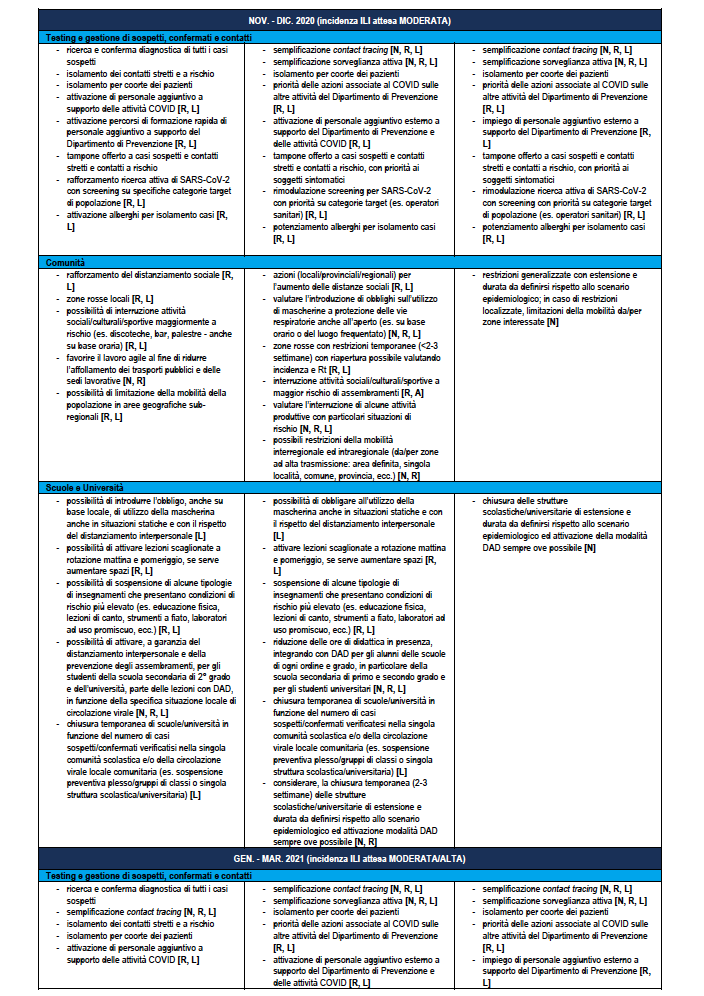
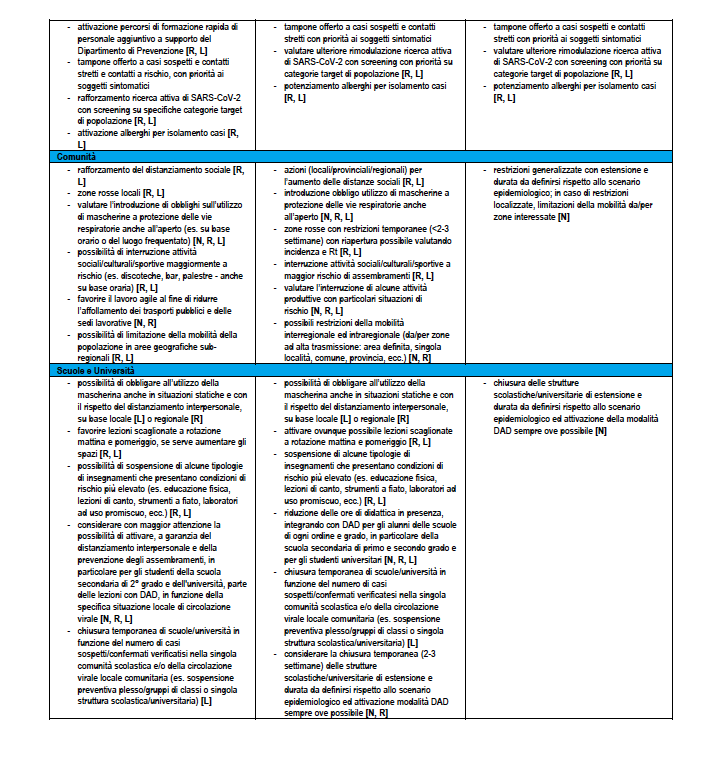
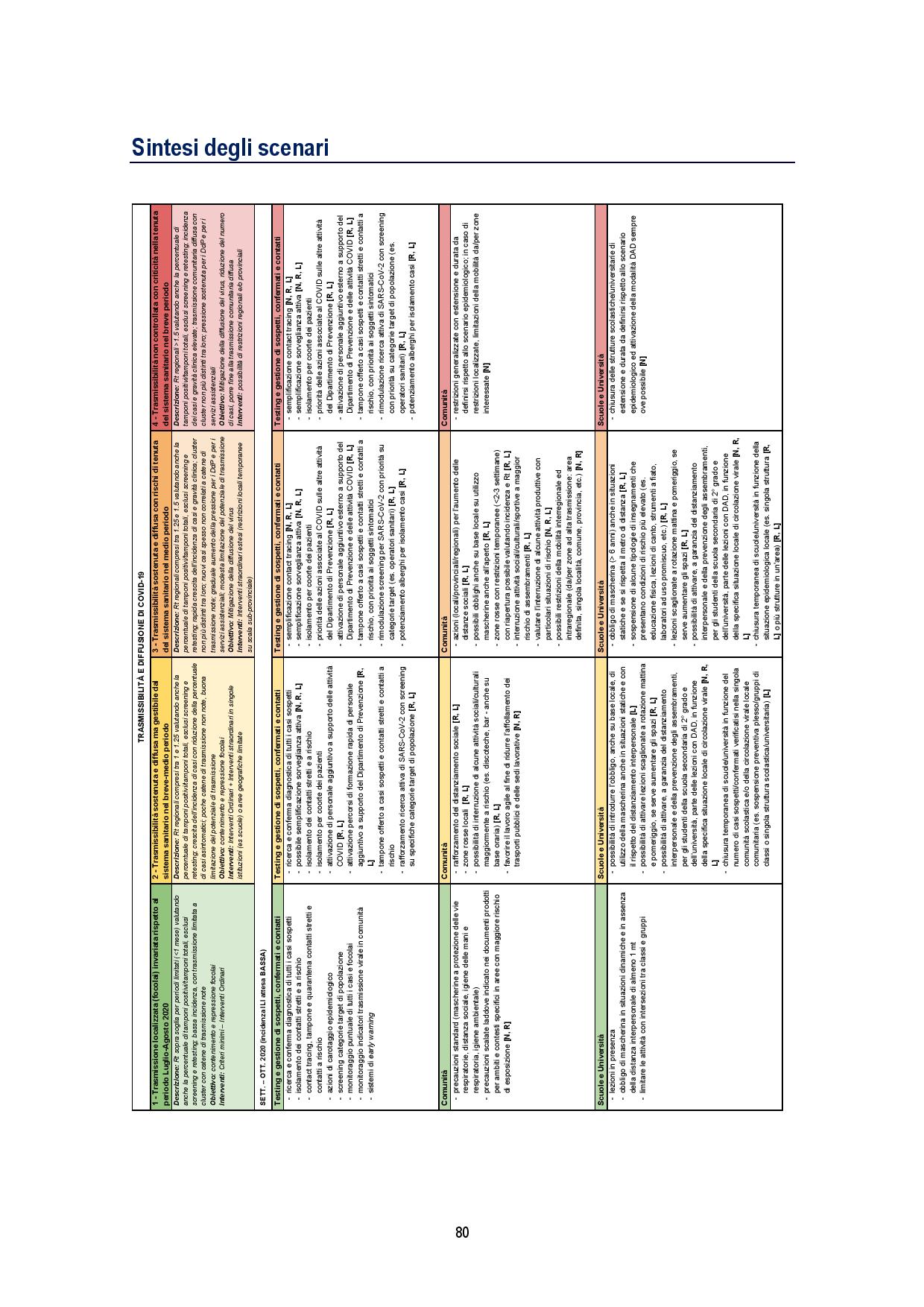
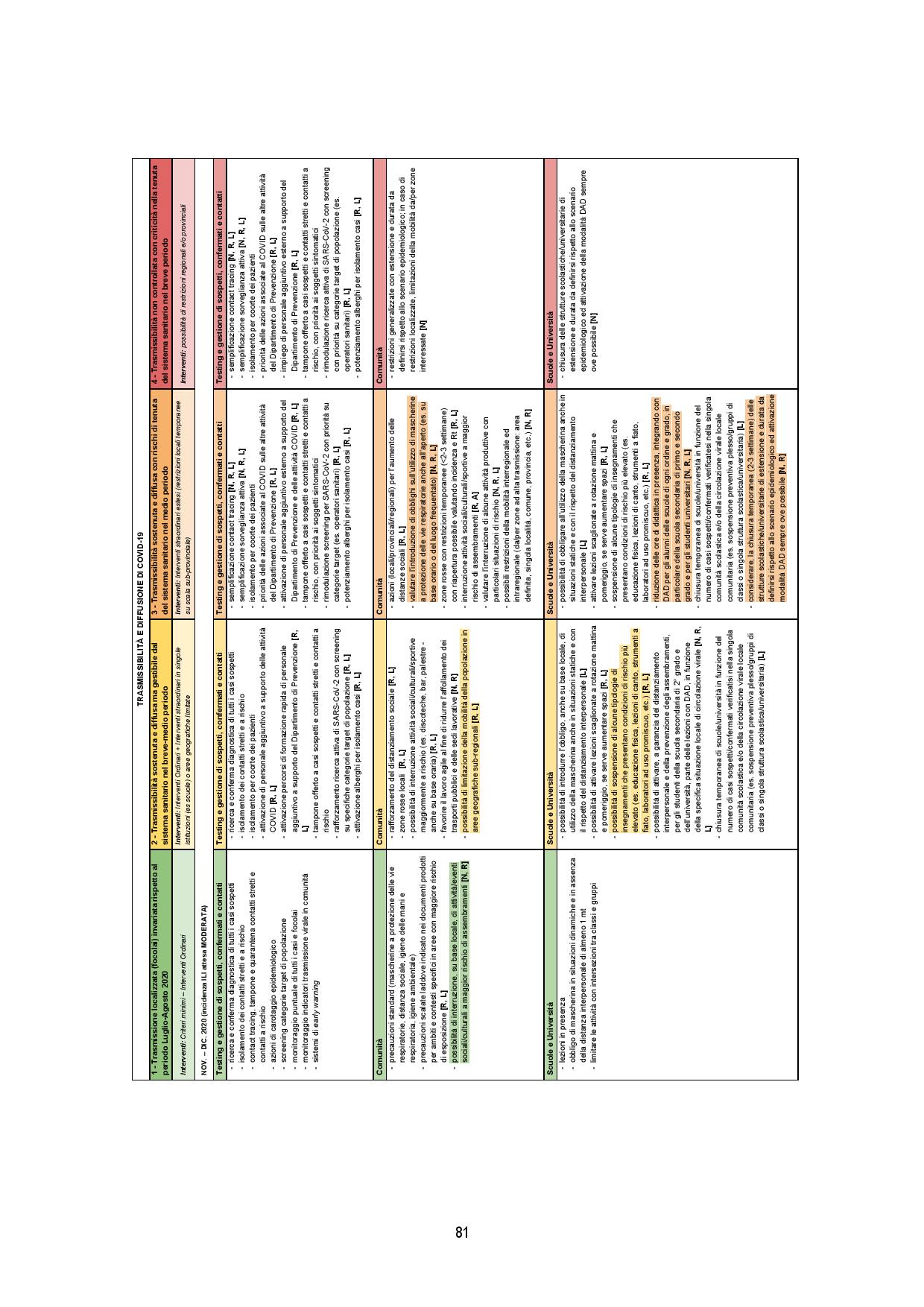
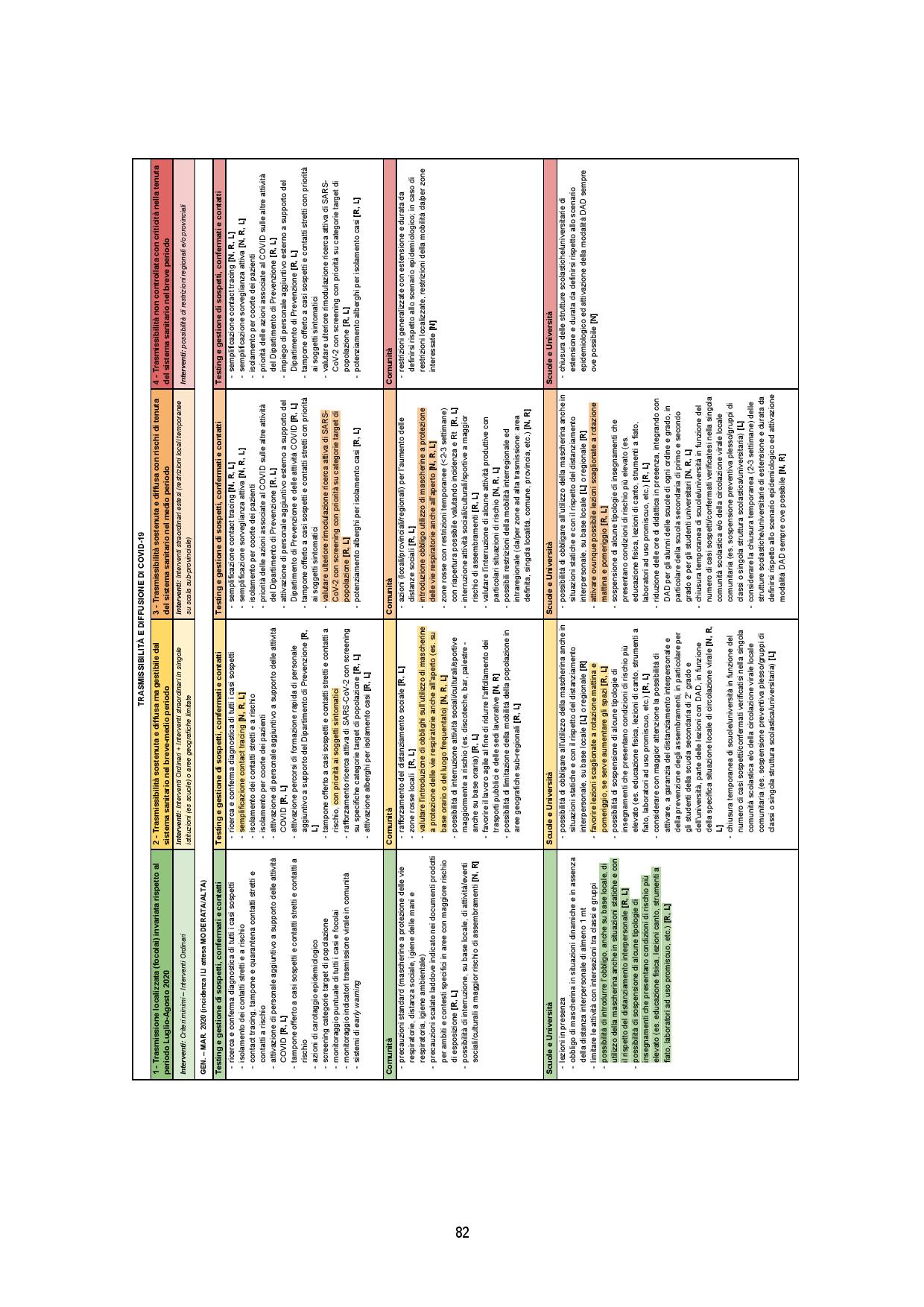
Table 4 reports the same re-modulation with declination of a detail of the re-modulation of the territorial measures at regional level, also considering the period of the year which is relevant for the different expected incidence of flu-like syndromes – ILI of various etiology (eg influenza viruses) that will impact health services simultaneously. The table gives indications on the actors involved where N: Central National Level; R: Regional Level; L: Local Level.
SCENARIO 2. Situation of sustained and widespread transmissibility but manageable by the health system in the short-medium term
Scenario description 2
Regional Rt values mainly and significantly comprised between Rt = 1 and Rt = 1.25 (i.e. with estimates of the 95% CI of Rt between 1 and 1.25), in the event that it is not possible to completely keep track of the new outbreaks, including school ones, but it is still possible to greatly limit the transmission potential of SARS-CoV-2 with ordinary and extraordinary containment / mitigation measures. An epidemic with these characteristics of transmissibility could be characterized, in addition to the evident impossibility of containing all the outbreaks, by a constant increase in the incidence of cases (at least symptomatic ones; it is in fact possible that a reduction in the percentage of asymptomatic cases is observed identified with respect to the total given the impossibility of carrying out the epidemiological investigation for all new outbreaks) and corresponding hospitalizations and admissions to intensive care. However, the growth in the number of cases could be relatively slow, without leading to a significant overload of care services for at least 2-4 months.
In a national scenario of this type, it is presumable that many Regions / PAs are classified as moderate to high risk, even if low risk situations are possible, at least if it were to be able to limit transmissibility in areas with sustained transmission in a short period. thus limiting interregional transmission.
1. Weekly Risk Rating: LOW / VERY LOW for at least 3 consecutive weeks at a higher risk assessment
Action: re-modulation of activities with less stringent measures (de-escalation) or maintenance
Interventions: ordinary, including:
• Case isolation
• Contact quarantine
• Standard precautions (PPE, physical distancing, individual / environmental hygiene) defined by the competent institutions (CTS, Ministries, ISS, INAIL etc.).
2. Risk classification: MODERATE
Action: evaluate the re-modulation of activities with more stringent measures (escalation) or maintenance
Risk assessment in the Region / PA to define sub-regional situations of higher risk (circulation in the provinces / municipalities; school outbreaks)
Interventions: ordinary + extraordinary in single institutions (eg schools) or limited geographical areas
• Greater control of the actual implementation of the measures already adopted on the territory (see minimum criteria)
• Scaled precautions where indicated in the documents produced for specific areas and contexts (eg schools) only in areas with greater risk of exposure
• Possibility of closure of activities, suspension of events and limitation of population mobility in sub-regional geographical areas (municipalities / provinces)
3. Weekly Risk Rating: HIGH / VERY HIGH (for less than 3 consecutive weeks)
Action: evaluate the re-modulation of activities with more stringent measures (escalation)
Interventions: extended overtime (temporary local restrictions on a sub-provincial scale)
• Physical distancing: eg. closing night clubs, bars, restaurants (initially potentially only at specific times – eg in the evening / night in order to avoid the "nightlife")
• School / university closure (incremental: class, plexus, on a geographical basis based on the epidemiological situation)
• Mobility limitations (to / from high transmission areas and possible restoration of agile work in specific areas.
• Temporary local restrictions on a sub-provincial scale (red zones) for at least 3 weeks with careful monitoring during the reopening phase. If a relatively low incidence is not maintained and Rt <1.2 in the mean value for at least 3 weeks after reopening, assess the need for restoration with possible geographical extension.
If a High / Very High risk classification persists for more than 3 consecutive weeks and evidence of a situation that cannot be managed with the extraordinary measures already in place, evaluate the response options in the subsequent scenarios.
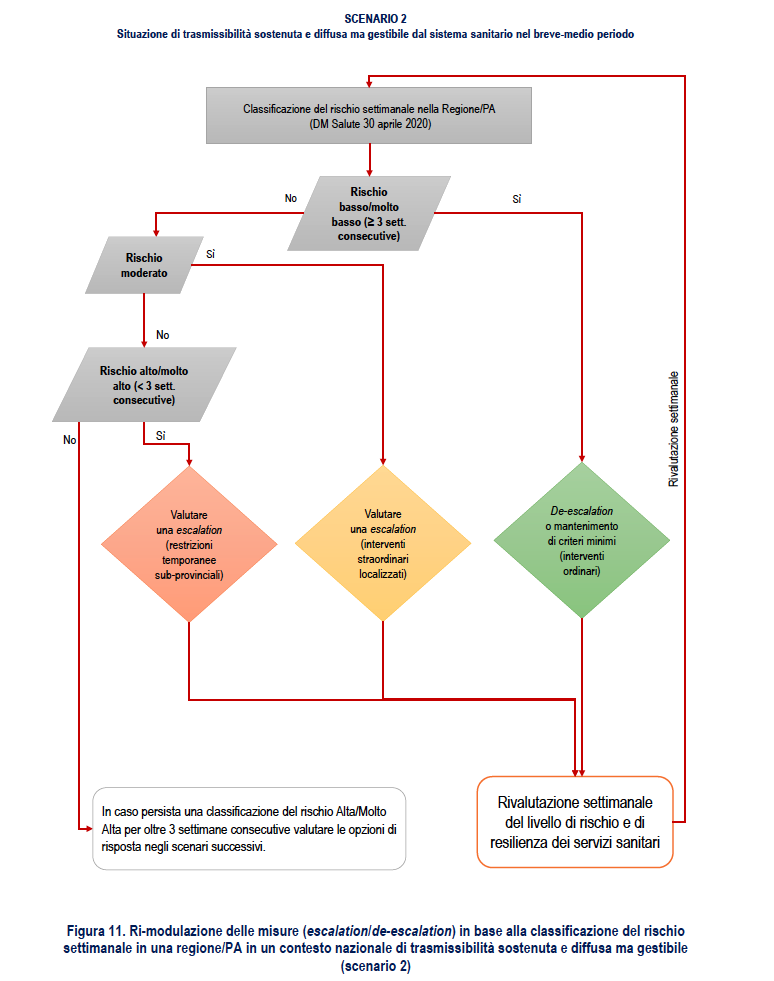
Figure 11 proposes a flow chart relating to the re-modulation of the measures based on the weekly classification of the risk in a Region / PA.
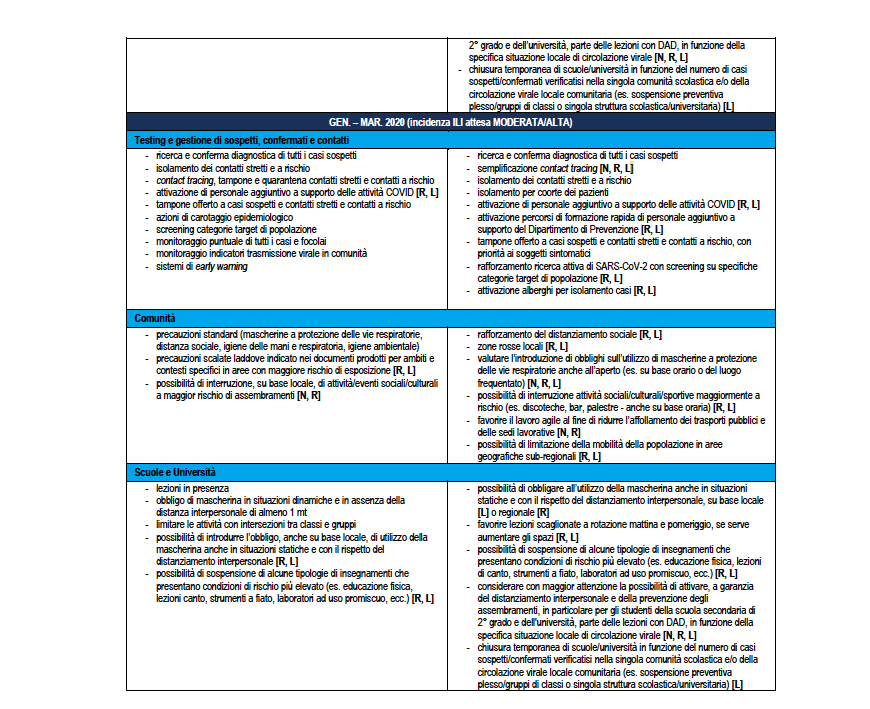
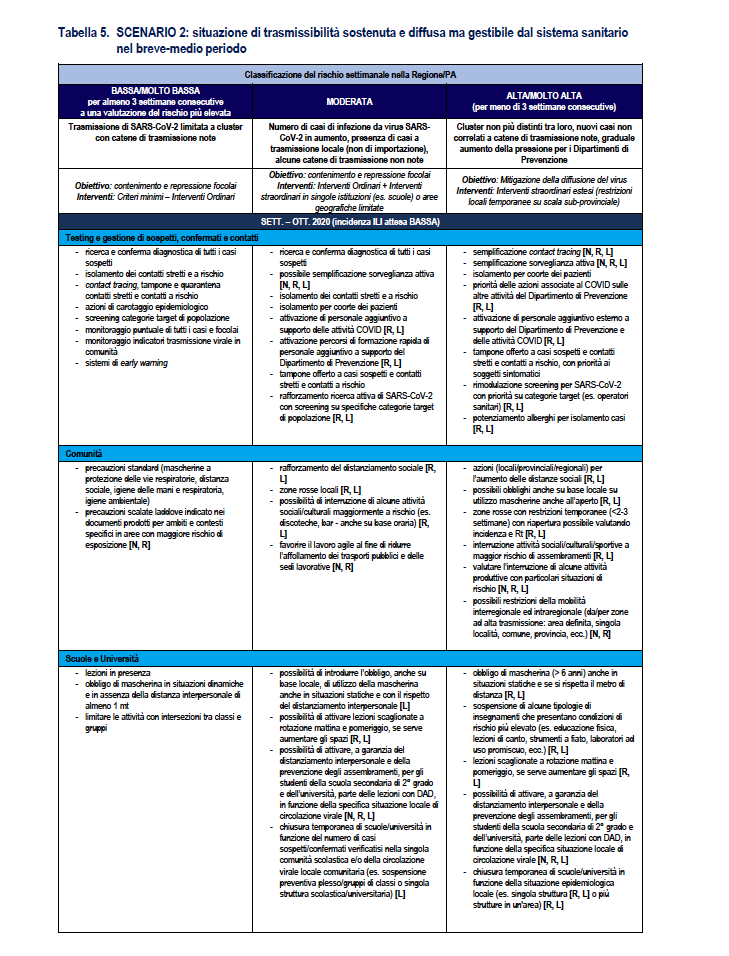
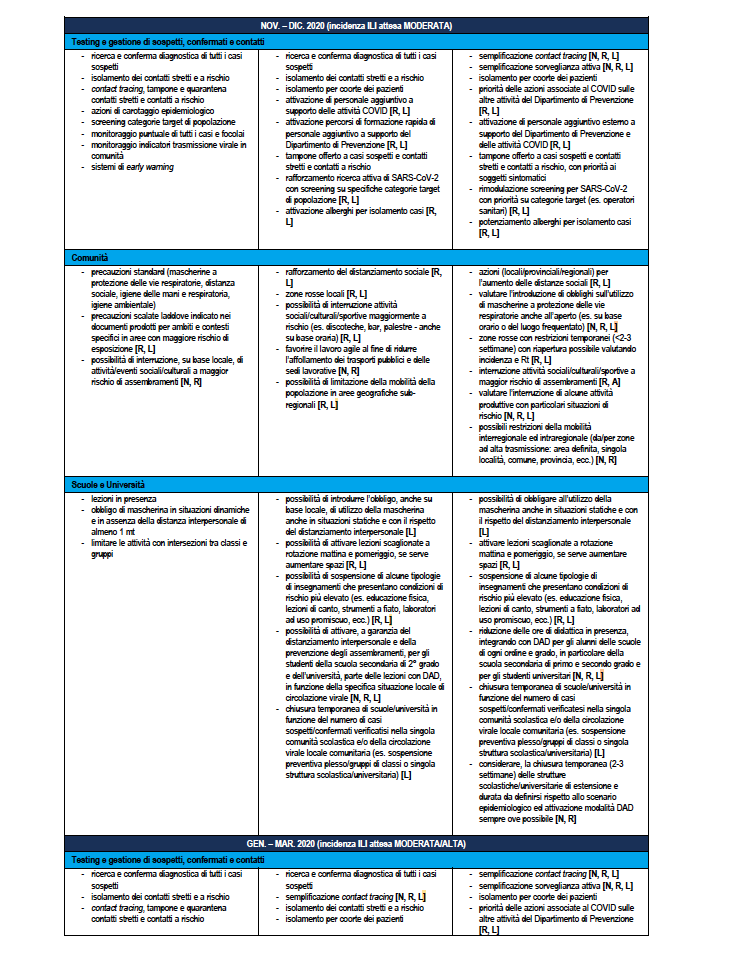
Table 5 reports the same re-modulation with declination of a detail of the re-modulation of the territorial measures at regional level also considering the period of the year which is relevant for the different expected incidence of flu-like syndromes – ILI (Influenza -like Illnesses) of various etiologies (e.g. influenza viruses) which will simultaneously impact health services. The table gives indications on the actors involved where N: Central National Level; R: Regional Level; L: Local Level.
SCENARIO 3. Situation of sustained and widespread transmissibility with risks of the health system in the medium term
Scenario description 3
Regional Rt values mainly and significantly comprised between Rt = 1.25 and Rt = 1.5 (i.e. with 95% CI estimates of Rt between 1.25 and 1.5), and in which it is possible to limit only modestly the transmission potential of SARS-CoV-2 with ordinary and extraordinary containment / mitigation measures. An epidemic with these transmissibility characteristics is expected to be characterized by a faster growth in the incidence of cases than in scenario 2), a failure to track chains of transmission, and initial signs of overload of care services following the increase in cases of high clinical severity (with an increase in the occupancy rates of hospital beds – critical and non-critical area) attributable to a high or very high risk level based on the monitoring system detected pursuant to the Health Ministerial Decree of 30 April 2020. The growth in the number of cases could lead to an overload of care services within 2-3 months. However, it is important to note that if the epidemic were to spread mainly among the younger age groups, as observed in the period July-August 2020, and it was possible to protect the most fragile categories (e.g. the elderly), the time margin within which to intervene could also lengthen a lot.
In a national scenario of this type it is presumable that many Regions / PAs are classified as high risk, even if lower risk situations are possible, at least if it were to be able to limit transmissibility in areas with sustained transmission in a short period, thus limiting interregional transmission. Should the high risk situation persist for a period of more than three weeks, more aggressive containment measures are most likely required.
1. Weekly risk classification: LOW / VERY LOW for at least 4 consecutive weeks based on a re-evaluation of consolidated data in order to reduce the risk of an underestimation of the risk due to a delay in the notification / transmission of surveillance data
Action: cautious re-modulation of activities with less stringent measures (de-escalation) if conditionally increased or maintenance
Interventions: ordinary, including:
• Case isolation
• Contact quarantine
• Standard precautions (PPE, physical distancing, individual / environmental hygiene) defined by the competent institutions (CTS, Ministries, ISS, INAIL etc.).
2. Weekly risk classification: MODERATE PERSISTENT or for at least 4 consecutive weeks based on a re-evaluation of the consolidated data in order to reduce the risk of an underestimation of the risk due to a delay in the notification / transmission of surveillance data
Action: evaluate the re-modulation of activities with more stringent measures (escalation) or maintenance
Risk assessment in the Region / PA to define sub-regional situations of higher risk (circulation in the provinces / municipalities; school outbreaks)
Interventions: ordinary + Extraordinary interventions in single institutions (eg schools) or limited geographical areas
• Greater control of the actual implementation of the measures already adopted on the territory (see minimum criteria)
• Scaled precautions where indicated in the documents produced for specific areas and contexts (eg schools) only in areas with greater risk of exposure
• Possibility of closure of activities, suspension of events and limitation of population mobility in sub-regional geographical areas (municipalities / provinces)
3. Weekly Risk Rating: HIGH / VERY HIGH (for less than 3 consecutive weeks)
Action: evaluate the re-modulation of activities with more stringent measures (escalation)
Interventions: extended overtime (temporary local restrictions on a sub-provincial scale)
• Physical distancing: eg. closing night clubs, bars, restaurants (initially potentially only at specific times, eg in the evening / night in order to avoid the "nightlife")
• School / university closure (incremental: class, plexus, on a geographical basis based on the epidemiological situation)
• Mobility limitations (to / from high transmission areas and possible restoration of agile work in specific areas.
• Temporary local restrictions on a sub-provincial scale (red zones) for at least 3 weeks with careful monitoring during the reopening phase. If a relatively low incidence is not maintained and Rt <1.2 in the mean value for at least 3 weeks after reopening, assess the need for restoration with possible geographical extension.
4. Weekly risk classification: HIGH / VERY HIGH (for 3 or more consecutive weeks) and evidence of a situation that cannot be managed with the extraordinary measures already in place
Action: Consider the possibility of Regional / Provincial restrictions
• Define a more extensive form of restriction on a Provincial or Regional scale based on the epidemiological situation
• Large-scale restoration of agile work and limiting individual mobility
Interventions: extraordinary (Table 6)
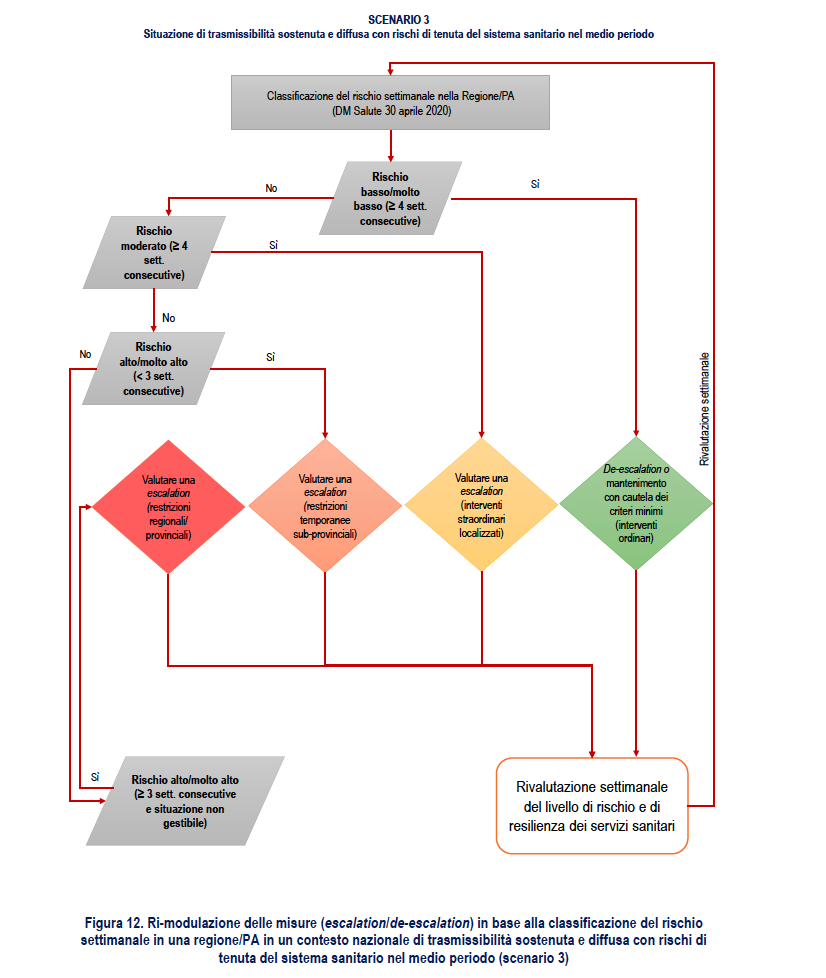
Figure 12 proposes a flow chart relating to the re-modulation of the measures based on the weekly classification of the risk in a Region / PA.
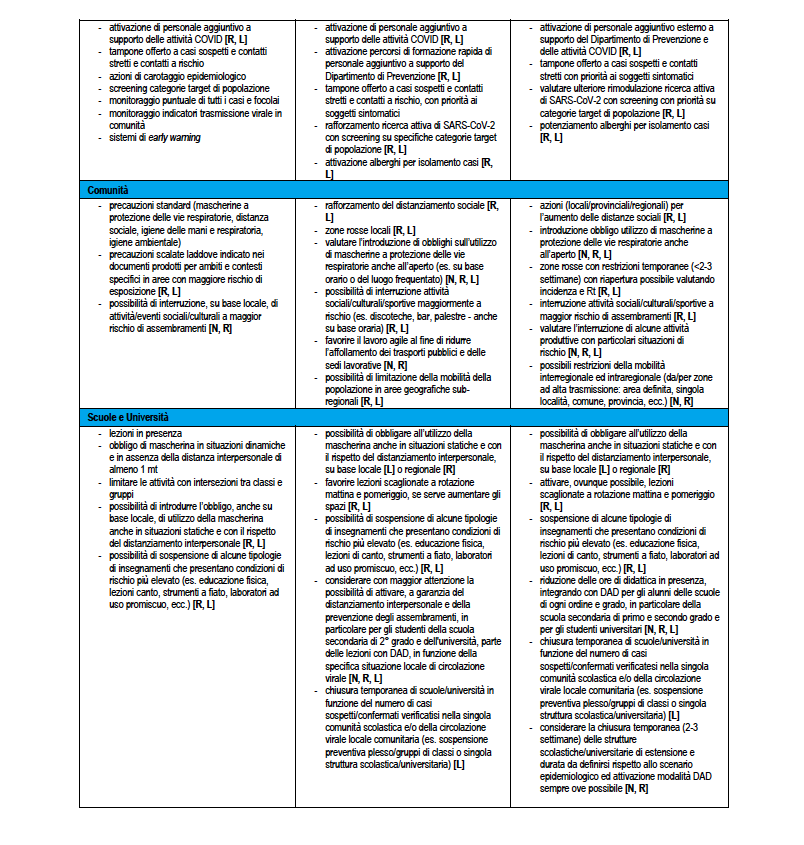
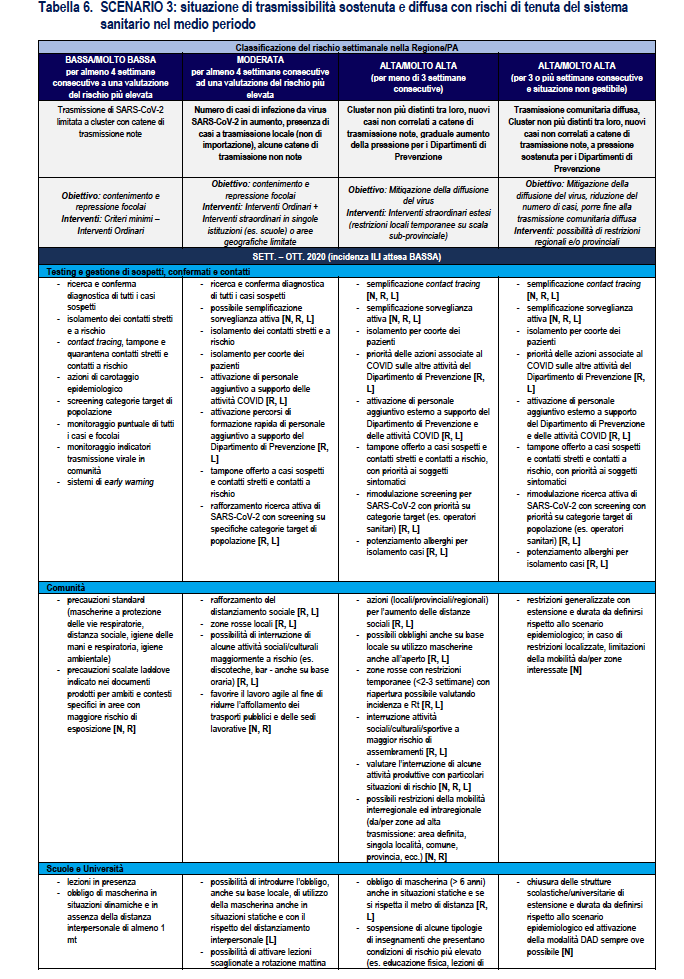
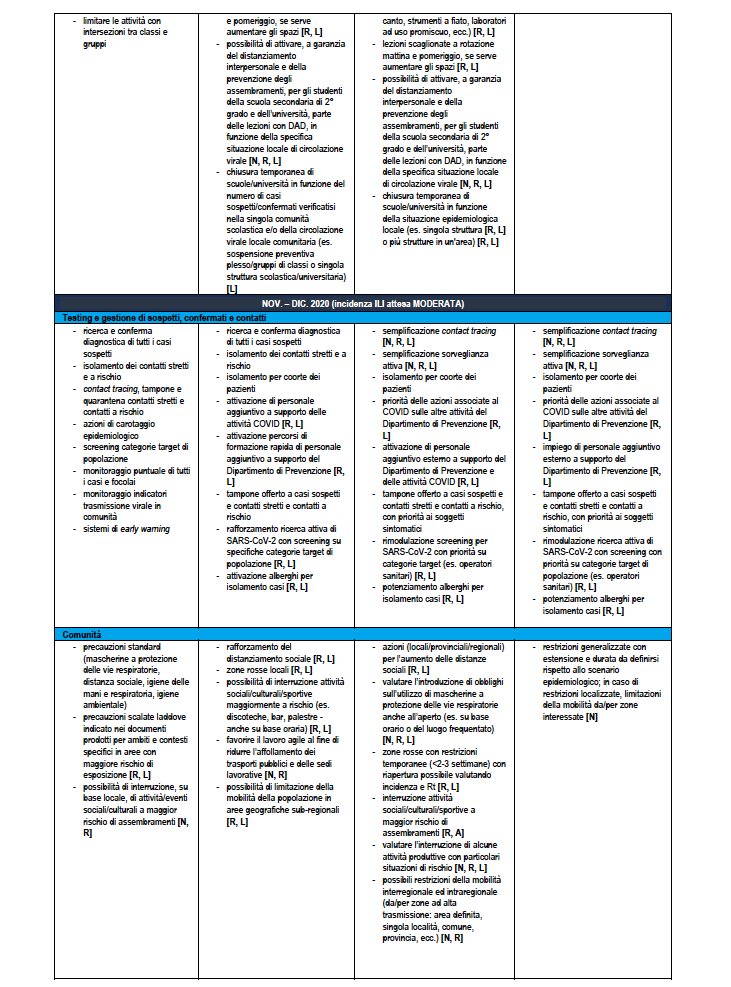
Table 6 reports the same re-modulation with declination of a detail of the re-modulation of the territorial measures at regional level also considering the period of the year which is relevant for the different expected incidence of flu-like syndromes – ILI (Influenza -like Illnesses) of various etiologies (e.g. influenza viruses) which will simultaneously impact health services. The table gives indications on the actors involved where N: Central National Level; R: Regional Level; L: Local Level.
SCENARIO 4. Situation of uncontrolled transmissibility with criticality in the health system in the short term
Scenario description 4
Regional Rt values predominantly and significantly greater than 1.5 (i.e. with estimates of 95% CI of Rt greater than 1.5). Such a scenario could quickly lead to a high number of cases and clear signs of overload of care services, without the possibility of tracing the origin of the new cases. The growth in the number of cases could lead to an overload of care services within 1-1.5 months, unless the epidemic spreads predominantly among the younger age groups, as observed in the period July-August 2020, and managed to protect the most fragile categories (eg the elderly). In this regard, it should be noted that it appears rather unlikely to be able to protect the most fragile categories in the presence of an epidemic characterized by these values of transmissibility.
In a national scenario of this type, it is presumable that many Regions / PAs are classified as high risk and, given the speed of diffusion and the interconnection between the various Regions / PAs, it is unlikely that there are situations of lower than moderate risk. If the high-risk situation persists for a period of more than three weeks, very aggressive containment measures are most likely required.
1. Weekly risk classification: MODERATE for at least 4 consecutive weeks based on a re-evaluation of consolidated data in order to reduce the risk of an underestimation of the risk due to a delay in the notification / transmission of surveillance data
Action: evaluate the re-modulation of activities with more stringent measures (escalation) or cautious maintenance or re-modulation of activities with less stringent measures (de-escalation) if previously increased in high / very high risk situations
Risk assessment in the Region / PA to define sub-regional situations of higher risk (circulation in the provinces / municipalities; school outbreaks)
Interventions: ordinary + extraordinary in single institutions (eg schools) or limited geographical areas
• Greater control of the actual implementation of the measures already adopted on the territory (see minimum criteria)
• Scaled precautions where indicated in the documents produced for specific areas and contexts (eg schools) only in areas with greater risk of exposure
• Possibility of closure of activities, suspension of events and limitation of population mobility in sub-regional geographical areas (municipalities / provinces)
2. Weekly Risk Rating: HIGH / VERY HIGH (for less than 3 consecutive weeks)
Action: evaluate the re-modulation of activities with more stringent measures (escalation)
Interventions: extended overtime (temporary local restrictions on a sub-provincial scale)
• Physical distancing: eg. closing night clubs, bars, restaurants (initially potentially only at specific times, eg in the evening / night in order to avoid the "nightlife")
• School / university closure (incremental: class, plexus, on a geographical basis based on the epidemiological situation)
• Mobility limitations (to / from high transmission areas and possible restoration of agile work in specific areas.
• Temporary local restrictions on a sub-provincial scale (red zones) for at least 3 weeks with careful monitoring during the reopening phase. If a relatively low incidence is not maintained and Rt <1.2 in the mean value for at least 3 weeks after reopening, assess the need for restoration with possible geographical extension.
3. Weekly risk classification: HIGH / VERY HIGH (for 3 or more consecutive weeks) and evidence of a situation that cannot be managed with the extraordinary measures already implemented
Action: Consider the possibility of regional / provincial extended restrictions
• Define a more extensive form of restriction on a Provincial or Regional scale based on the epidemiological situation
• Large-scale restoration of agile work and limiting individual mobility.
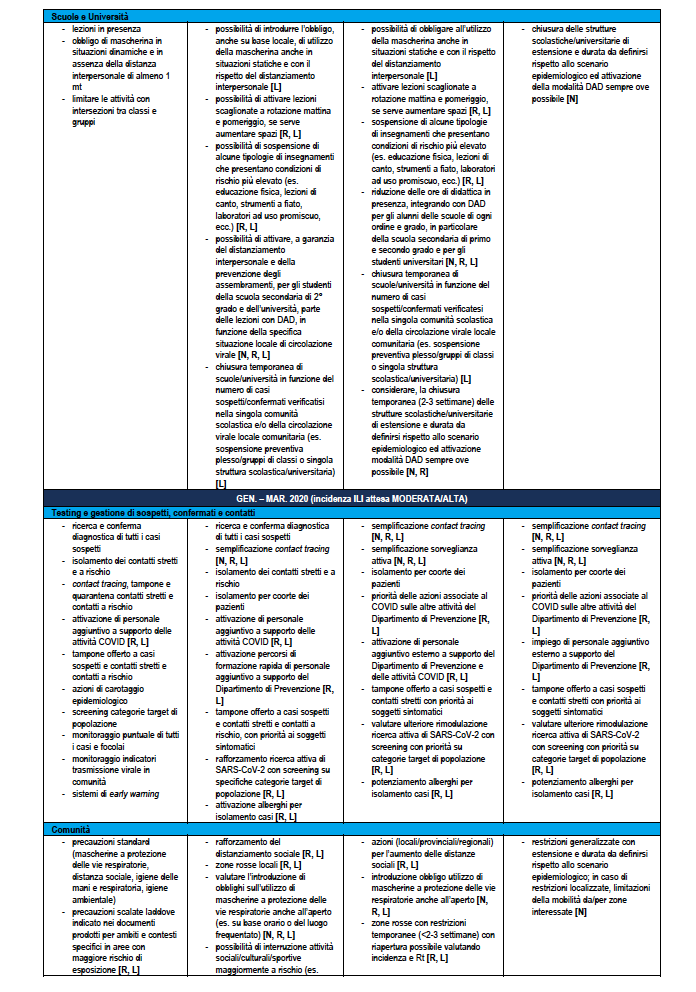
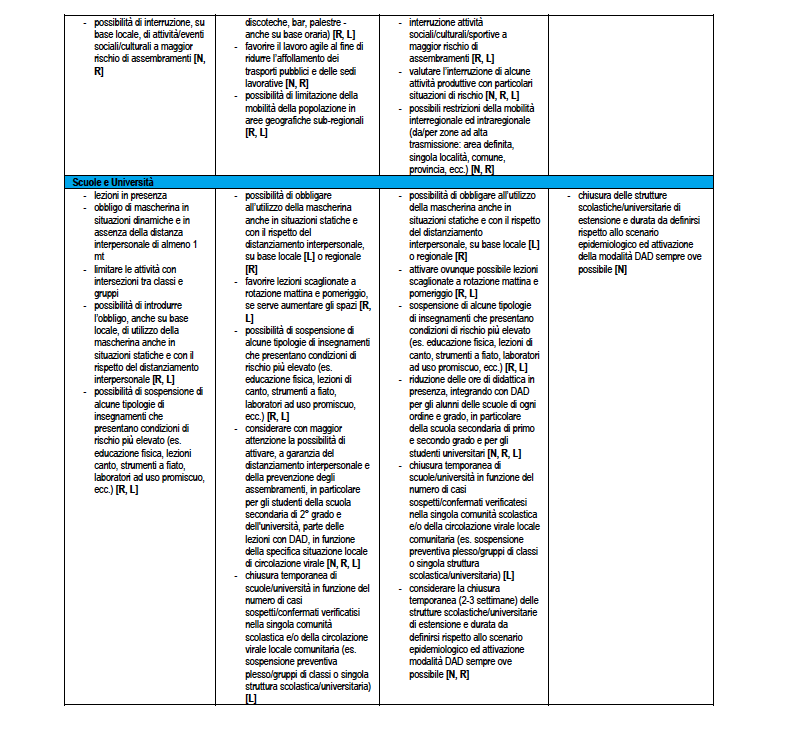
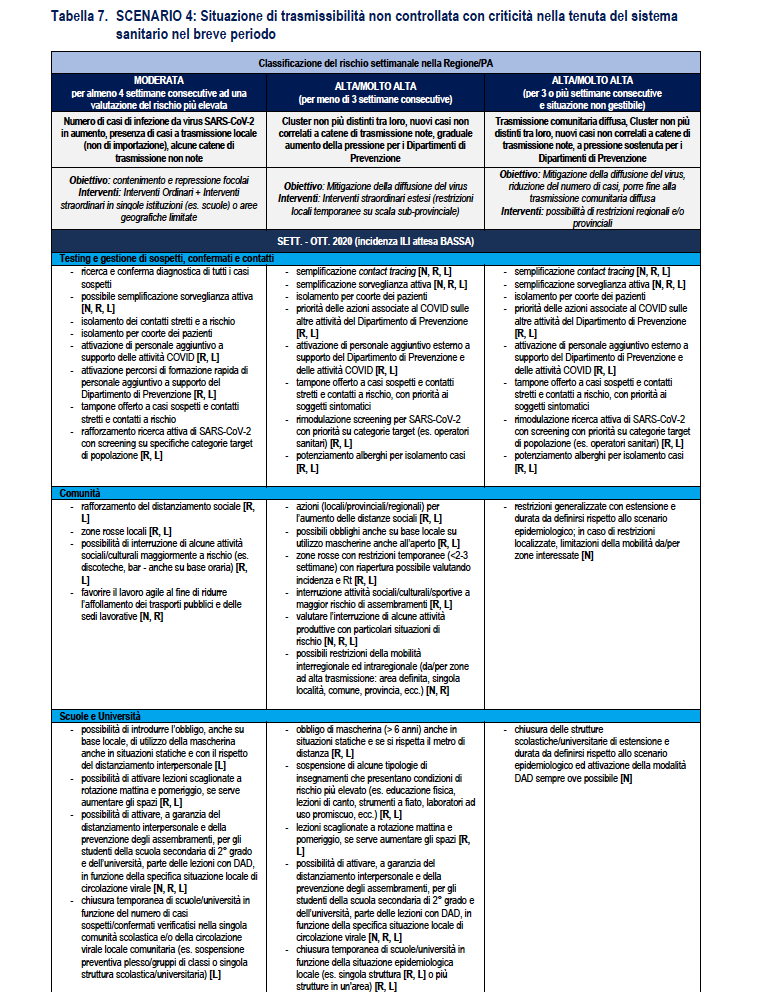
Interventions: extraordinary (Table 7)
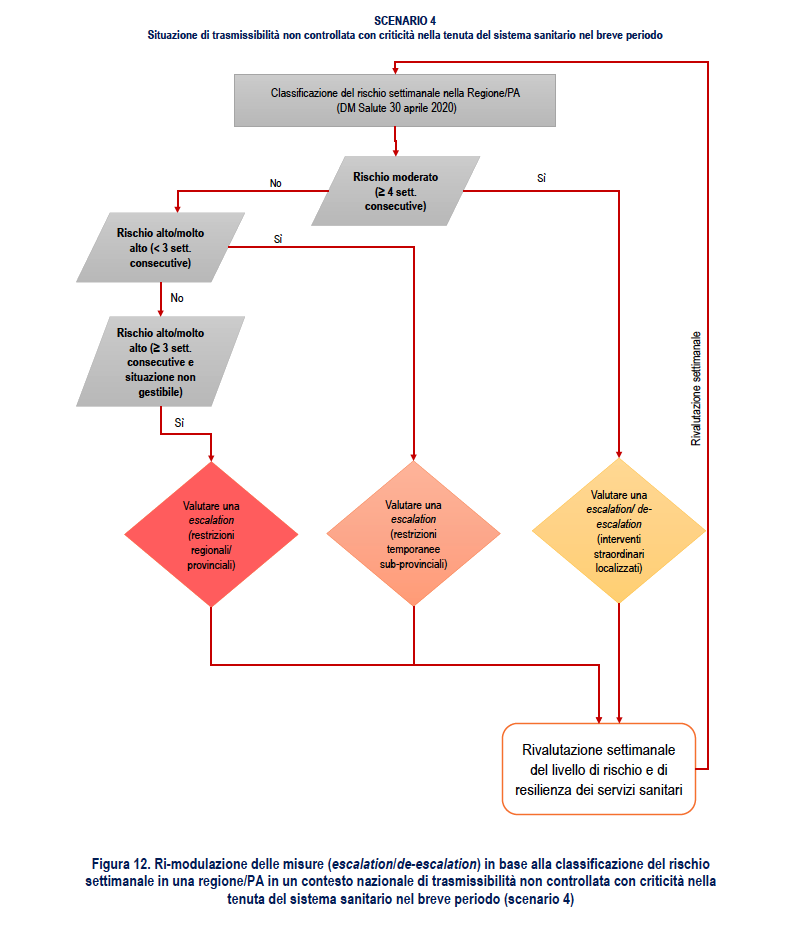
Figure 12 proposes a flow chart relating to the re-modulation of the measures based on the weekly classification of the risk in a Region / PA.
Table 7 reports the same re-modulation with declination of a detail of the re-modulation of the territorial measures at regional level also considering the period of the year which is relevant for the different expected incidence of flu-like syndromes – ILI (Influenza -like Illnesses) of various etiologies (e.g. influenza viruses) which will simultaneously impact health services. The table gives indications on the actors involved where N: Central National Level; R: Regional Level; L: Local Level.
This is a machine translation from Italian language of a post published on Start Magazine at the URL https://www.startmag.it/mondo/sars-cov-2-che-cosa-succedera-in-autunno-inverno-report-iss-ministero-salute/ on Mon, 12 Oct 2020 14:25:25 +0000.